




| Original Research | ||
Natl. J. Physiol. Pharm. Pharmacol. (2025), Vol. 15(2): 128-136 Research Article Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospitalHiren Jitendra Udhnawala1*, Nazima Mirza1, Nirav Asarawala2 and Barna Ganguly1 1Department of Pharmacology, Pramukh Swami Medical College, Karamsad, India 2Department of Oncology, Pramukh Swami Medical College, Karamsad, India *Corresponding Author: Hiren Jitendra Udhnawala. Department of Pharmacology, Pramukh Swami Medical College, Karamsad, India. Email: hirenju [at] charutarhealth.org Submitted: 16/10/2024 Accepted: 01/01/2025 Published: 28/02/2025 © 2025 Natl. J. Physiol. Pharm. Pharmacol
ABSTRACTBackground: Cisplatin is a commonly used chemotherapy agent for solid tumors, including lung, ovarian, testicular, bladder, and oral cancers. However, it can cause significant adverse drug reactions (ADRs). Therefore, this study aimed to evaluate the experience of patients with cancer undergoing chemotherapy by estimating the number of ADRs associated with cisplatin treatment. Materials and Methods: Prospective observational research was conducted in a hospital setting by the Department of Pharmacology in collaboration with the Department of Oncology in Shree Krishna Hospital, Karamsad, Anand, Gujarat, from February 18, 2023, to February 29, 2024. The study included 105 patients at the daycare center who were receiving cisplatin-based chemotherapy for the first time for solid cancer tumors. Sample size calculation was done based on the number of patients admitted to daycare for cisplatin treatment. Results: Of the 105 participants, most (70.48%) were male, with a mean age of 49.03 years; the majority of them were receiving treatment for malignancies of the buccal mucosa and oral cavity. Cisplatin was administered according to the protocol, with antiemetic and hydration measures to mitigate adverse effects. Nephrotoxicity, tinnitus, vomiting, hearing loss, and loss of taste were notable ADRs among the study participants. Conclusion: ADRs, such as vomiting, nephrotoxicity, tinnitus, and loss of taste, were noted at different frequencies during each cycle. Most of the studies were mild but not preventable, and they had no impact on the patients’ course of therapy. Keywords: Cisplatin, adverse drug reaction (ADR). IntroductionCisplatin is an alkylating drug based on platinum that is effective against various solid tumor types, such as lung, ovarian, testicular, and bladder malignancies. Despite its effectiveness, cisplatin’s adverse reactions, which can range in severity from mild to severe, frequently restrict its clinical utility (Dasari and Bernard Tchounwou 2014). Because of its strong antitumor effects, cisplatin remains the mainstay in the management of numerous cancers such as solid tumors of the buccal mucosa, oral cavity, tongue, cervix, and oropharynx (Ranasinghe et al., 2022). Comprehending the ADR profile linked to cisplatin is crucial for guaranteeing patient safety and customizing treatment approaches to reduce toxicity while optimizing effectiveness (Khandelwal et al., 2015). Common adverse drug reactions (ADRs) of cisplatin include emesis despite the highly antiemetic drug given along with it. Nephrotoxicity, myelosuppression, ototoxicity, gastrointestinal toxicity, and neurotoxicity are the other ADRs (Barabas et al., 2008). Quality of life of the patients might be adversely affected by these side effects, which can have a major influence on social functioning, mental stability, and physical health (Megari 2013). Cisplatin’s most well-researched adverse drug reaction is nephrotoxicity (McSweeney et al., 2021). Ototoxicity is a noteworthy issue that presents substantial difficulties for sensory functioning and communication capacities in patients. It can cause irreversible hearing loss and tinnitus (Ganesan et al., 2018). The symptoms of gastrointestinal toxicity, which include nausea, vomiting, and mucositis, can have a significant impact on dietary consumption, fluid status, and treatment compliance, ultimately jeopardizing the general health of patients (Makrilia et al., 2010). Myelosuppression increases the risk of infections, bleeding, and fatigue. The condition is characterized by leukopenia, thrombocytopenia, and anemia. As a result, meticulous hematological monitoring and supportive care measures. Furthermore, cisplatin hypersensitivity reactions might cause urticaria, bronchospasm, or anaphylaxis, which means that they need to be identified and treated immediately to avoid serious allergic side effects (Makrilia et al., 2010). Healthcare practitioners can optimize treatment regimens, implement proactive symptom management measures, and improve patient-centered care delivery by methodically evaluating the occurrence, severity, and effect of ADRs associated with chemotherapy with cisplatin. The need for studies on ADRs due to cisplatin in cancer chemotherapy arises from several critical factors such as patient safety and well-being, treatment optimization, clinical evaluation and selection, and research advancement. This approach can help identify potential opportunities for improving cancer care and improving overall health during chemotherapy. By collaborating with physicians, researchers, and patients, it is necessary to enhance overall therapeutic outcomes for patients with cancer and further our understanding of toxicity related to cisplatin. AimThis study evaluated the burden of ADRs associated with cisplatin therapy to evaluate the experience of patients with cancer undergoing chemotherapy. ObjectiveTo assess the frequency and severity of cisplatin-related adverse drug reactions in patients with cancer. Materials and MethodsThis studyThe prospective observational research in a hospital setting was conducted by the Department of Pharmacology in collaboration with the Department of Oncology in Shree Krishna Hospital, Karamsad, Anand, Gujarat, during 18th February 2023 to 29th February 2024. Ethical clearanceThe study (Ref.no. 10/68/2023) was approved on 16/02/2023 by the Institutional Ethics Committee on February 16, 2023. Sample sizePatients who were taking cisplatin-based chemotherapy for the first time for solid cancer tumors at the daycare center during the study period were included in the study. Sample size calculation was done based on the number of patients admitted to daycare for cisplatin treatment. The total sample size was 105 patients. Inclusion criteria
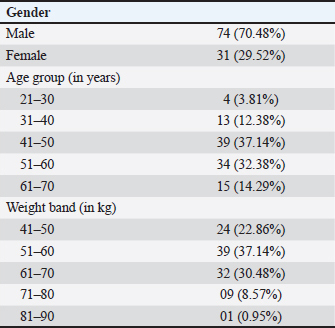
Exclusion criteria
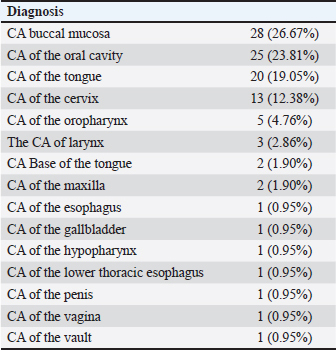
Data were collected from the oncology department and entered the case record form (CRF). Details of various ADRs during each cycle of cisplatin-based chemotherapy were noted. The severity and preventability of ADRs were assessed using the Hartwig & Siegel ADR Severity Assessment scale (Hartwig et al., 1992) and modified Schumock–Thornton criteria (Bellare et al., 2016). The severity of vomiting was graded based on the nausea and vomiting grading scale NCI CTCAE (Version 4.03) (Gahart et al., 2016). Each patient was followed up for 4 cycles or at least consecutive 2 cycles as per respective chemotherapy. A simple patient-friendly diary was developed to note down the adverse effects between doses or cycles by the patient themselves or relatives. On the first day of the next cycle, the diary data were reviewed and recorded in the CRF. All the data were collected, compiled, and analyzed using Microsoft Excel 2019. Microsoft Excel was used to generate graphs and tables. Descriptive statistics, such as mean, SD, range, percentage, and frequency, were used to describe the data. ResultData of 105 study patients as per inclusion criteria, who were receiving cisplatin therapy, were collected. All patients were attending daycare. At the end of the study, seven patients were lost to follow-up. Demographic characteristics of the participantsThere were 70.48% (n=74) males and 29.52% (n=31) females in the study. The mean age of the participants was 49.03 ± 10.35 years. Almost 37.14% belonged to the 41–50 years age group followed by 51–60 years (32.38%, n=34), 61–70 years (14.29%, n=15), 31–40 years (12.38%, n=13), and 21–30 years (3.81%, n= 4). The mean weight of study participants was 57.75 ± 8.94 kilograms. Nearly 37.14% (n=39) of study participants had weight 51–60 kg followed by 61–70 kg (30.48%, n=32), 41–50 kg (22.86%, n=24), 71–80 kg (8.57%, n=9), and only one (0.95%) weighted 81–90 kg (Table 1). Nearly one-fourth of the total participants (26.67%, n=28) were diagnosed with CA buccal mucosa, and the other one-fourth (23.81%, n=25) had CA oral cavity. Thus, the highest proportion was noted for oral cavity cancers. The CA tongue had a high distribution (19.05%, n=20). CA cervix was noted among 12.38% (n=13) of participants. Other carcinomas were oropharynx (4.76%, n=5), larynx (2.86%, n=3), base of tongue (1.90%, n=2), maxilla (1.90%, n =2), esophagus (0.95%, n=1), gallbladder (0.95%, n=1), hypopharynx (0.95%, n=1), lower thoracic esophagus (0.95%, n=1), penis (0.95%, n=1), vagina (0.95%, n =1), and vault (0.95%, n=1) (Table 2). Cisplatin therapyOut of the total study participants, most of them (97.14%) were on Inj Cisplatin (weekly cycle), while some of them (1.90%) were on Inj Cisplatin + Methotrexate (monthly cycle) and Inj Cisplatin + Inj Gemcitabine (0.95%) (every 21-day cycle). Also, adjuvant therapies, such as Inj Granisetron 3 mg, Inj Dexamethasone 12 mg, Inj MgSo4 2 ampule, and Inj KCL 1 ampules, were given to almost all patients before cisplatin chemotherapy to prevent vomiting and other side effects according to protocol. Three groups of patients had different combinations. In the group where Inj Cisplatin and other adjuvant drugs were administered, each patient was receiving 4.04 ± 0.49 drugs in each cycle. In the other groups with Inj Cisplatin + Methotraxete, the mean was found to be 4 ± 0.002/cycle, and in the group with Inj Cisplatin + Inj Gemcitabine 1.6 gm, the mean was 5.5 ± 0.70 drugs/cycle. Table 1. Demography of study participants (N=105).
Table 2. Distribution of study participants according to diagnosis (N=105).
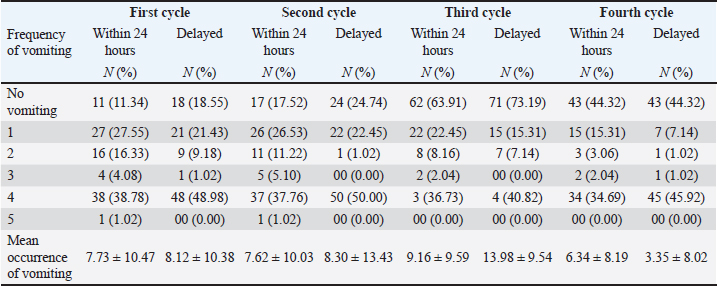
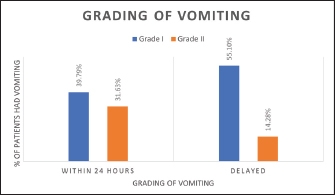
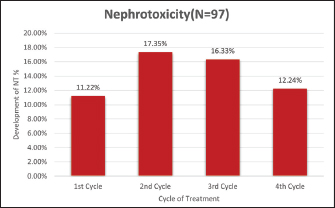
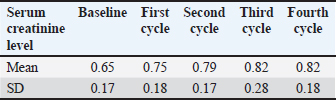
Adverse drug reactions of cisplatinVomiting According to the Symptom Management Guidelines (NCI GRADE AND MANAGEMENT), vomiting is defined as the forceful expulsion of stomach, duodenum, or jejunum contents through the oral cavity. Vomiting was graded from grade I (Mild)to Grade V (Death) according to the Nausea and Vomiting Scale NCI CTAE (Version 4.03). Grade I: 1 and 2 episodes (separated by 5 minutes) in 24 hours Grade II: 3–5 episodes (separated by 5 minutes) in 24 hours During the first cycle and within 24 hours, 27.55% (n =27) had vomited once,16.33% (n=16) had twice, 4.08% (n=04) vomited thrice, 38.78% (n=38) had 4 times, and 1.02% (n=1) had 5 times vomiting. During the second cycle and within 24 hours, 26.53% (n=26) had vomited once, 11.22% (n =11) vomited twice, 5.10% (n=5) vomited thrice, 37.76% (n=37) had 4 times, and 1.02% (n=1) had 5 times vomiting within 24 hours. During the third cycle and within 24 hours, 22.45% (n =22) had vomited once, 8.16% (n = 8) had vomited twice, 2.04% (n=2) had thrice, 36.73% (n = 36) had 4 times, and none had vomited more than that. During the fourth cycle and within 24 hours, 15.31% (n=15) had vomiting once, 3.06% (n=3) had twice, 2.04% (n=2) had three times, and 34.69% (n = 24) had 4 times (Table 3). Mean 7.73 ± 10.47 patients experienced vomiting within 24 hours of treatment in the first cycle. The mean frequency of patients was noted highest during the third cycle and lowest during the fourth cycle. As none of the patients had a vomiting frequency of >5, they had grade I and II vomiting. No patient experienced vomiting exceeding grade II. Nearly 39.79% vomited in grade I and 31.63% vomited in grade II within 24 hours of treatment. Delayed vomiting was observed in 69.38% of participants. Out of them, 55.10% vomited in grade I, whereas 14.28% vomited in grade II vomiting (Fig. 1). NephrotoxicityDrug-induced nephrotoxicity has been defined in the published literature as an increase of ≥0.5 mg/dl (or a 50% increase) in serum creatinine over the baseline level or a decrease in creatinine clearance of ≥ 50% from baseline on two consecutive days. During the first cycle, nephrotoxicity was noted among 11 (11.22%), while 17 (17.35%) developed during the second cycle and 16 (16.33%) and 12 (12.24%) developed during the third cycle and fourth cycle, respectively (Fig. 2). The mean serum creatinine level increases in successive cycles. Patients who developed nephrotoxicity in the first cycle had unremittingly high serum creatinine levels thereafter. However, some of the patients with deranged serum creatinine levels subsequently had normal levels. Thus, an overlap of patients was noted between the incidence of nephrotoxicity during subsequent cycles (Table 4). Table 3. Distribution of study participants according to frequency of vomiting (N=97).
Fig. 1. Distribution of study participants according to grading of vomiting (N=97).
Fig. 2. Distribution of study participants according to the development of nephrotoxicity during treatment. Table 4. Mean serum creatinine level during each cycle (N =97).
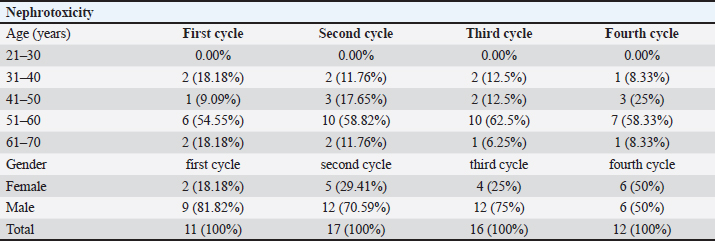
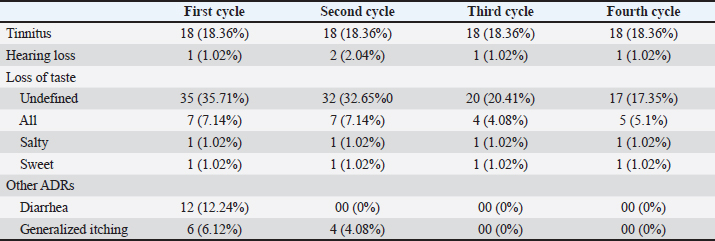
Those who developed nephrotoxicity during the first cycle 81.82% (n=9) were males. During the second cycle, 70.59% (n=12) were males, and during the third cycle, 75.00% (n=12) were males. An equal proportion of sex was noted during the fourth cycle among those who had nephrotoxicity. In the first cycle, 54.55% (n = 6) of patients with nephrotoxicity belonged to 51–60 years of age group followed by 31–40 years (18.18%), 61–70 years (18.18%), and 41–50 years (9.09%). During the second cycle, a similar proportion was noted. In the third cycle, the highest proportion was noted among 51–60 years and lowest among 61–70 years. In the last cycle, a lower proportion was noted among 31–40 years compared to other cycles. None of the younger participants (21–30 years) developed nephrotoxicity in any of the cycles (Table 5). Out of 98 participants 18.36% (n=18) developed tinnitus after the first cycle and the same continues at the end of the fourth cycle. The number of patients with tinnitus remained the same during each cycle, and no treatment was given for the tinnitus. Only a few patients developed bilateral hearing loss at the end of all cycles. Nearly, 71% developed undefined loss of taste. Out of them, 7.14% (n=7) had all types of loss of taste, while 1.02% (n=1) had a loss of taste of salt and 1.02% had sweet taste loss after the first cycle. At the end of fourth cycle, 24.49% (n=24) continued with some loss of taste. Therefore, it has been observed that an increase in the loss of taste was found in the initial two cycles, which later decreased in the subsequent cycles. Other ADRs, such as diarrhea (12.24%) and generalized itching (6.12% in the first cycle and 4.08% in the second cycle), were noted during treatment. These complaints were resolved at the end of fourth cycle (Table 6). Table 5. Nephrotoxicity and demography (N=97).
Table 6. Distribution of study participants according to the development of tinnitus, hearing loss, loss of taste, and other ADRs during treatment (N=97).
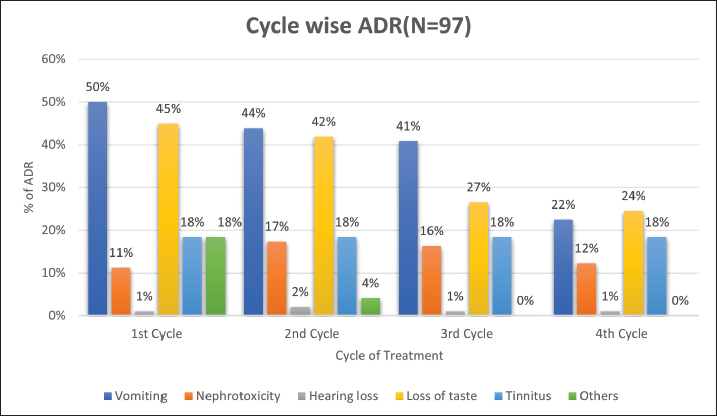
Figure 3 shows that during the first cycle, ADR-like nephrotoxicity (11.22%), hearing loss (1.02%), loss of taste (44.90%), tinnitus (18.37%), and others like generalized itching and diarrhea were noted. During the second cycle, the proportion of nephrotoxicity was increased (17.35%) and the incidence of vomiting was decreased. The loss of taste was improved during the third cycle, and at the end of the fourth cycle, the proportion of nephrotoxicity was the same, but the loss of taste (24.49%) and vomiting (22.45%) were decreased. Myelosuppression in the form of thrombocytopenia occurred in 39.79% of patients, resulting in a frequency of 39 patients. Preventability and severity of ADRsThe preventability of ADR was based on the event. Vomiting was definitely preventable among all patients (100%) because the administration of antiemetics with a cisplatin regimen can prevent ADR. Nephrotoxicity was probably preventable (100%), as noted for thrombocytopenia. Tinnitus, hearing loss, and loss of taste were not preventable. It was noted that out of the total events that occurred during the course of treatment with cisplatin therapy, they had various severity levels classified into levels 1 and 2 (mild), 3 and 4 (moderate), and 5, 6, and 7 (severe) according to Hartwig & Siegel ADR severity assessment. The vomiting frequency was noted as level 1 among 37.14%, level 2 among 24.29%, and level 3 among 38.57%. More than half (61.43%) of the patients noted nephrotoxicity as level 1, while 12.86% noted nephrotoxicity as level 2 and 25.71% noted nephrotoxicity as level 3. More than half (52.00%) of patients noted myelosuppression (thrombocytopenia) as level 1, while 22.00% noted it as level 2 and 26.00% noted it as level 3. For tinnitus, loss of taste and hearing loss 100% noted severity as level 1.
Fig. 3. Cycle-wise ADR. DiscussionAntineoplastic medications, such as cisplatin (cis-diamminedichloroplatinum (II), CDDP), are used to treat a variety of solid-organ malignancies, such as those of the breast, testis, ovary, lung, head, and neck. Cisplatin has several toxicities, including allergic reactions, myelosuppression, ototoxicity, gastrotoxicity, vomiting, and nephrotoxicity. Despite these adverse effects, no less toxic alternative has been found. Therefore, cisplatin remains a commonly prescribed chemotherapeutic agent for solid tumors, including head and neck cancers, testicular cancer, small-cell and non-small-cell lung cancer, and bladder cancer (Miller et al., 2010). Cancer diagnosis in the study participantsGlobally, oral and buccal cancers are among the most prevalent cancers in the world, and oral cancer is the sixth most common type of cancer. In addition, India is the second country with the highest number of oral cancer cases (Borse et al., 2020). Oral cancer is top three cancers prevalent in India, accounting for more than 30% of all cancer cases reported in the nation (Coelho 2012). The prevalence of cancer is also high in Gujarat, and among them, the highest proportion was noted for oral cavity and buccal mucosa cancers. Krishna et al. (2014) also noted a higher proportion of oral cavity cancers in their study. This finding accorded with the present study as the highest number of patients included was noted for oral cavity and buccal mucosa cancers (Khandelwal et al., 2015). Male participants (70.48%) dominated the present study, which coincides with the study conducted by Krishna et al. (2014) (90%). The mean age of the participants was 49.03 ± 10.35 years in the present study, and a similar result was noted by Aruna et al. (2011). The majority of the study participants belonged to the 41–60 years group, which indicates the highest prevalence of cancer in the middle-aged population in the present study that shows the same prevalence in the majority of study (Attia 2017; Zeb et al., 2008). In contrast, Gupta et al. (1996) noted a higher prevalence among 41–60 age group. In this study, the prevalence of cancer among 21–30 years of age was noted lower than that in the study conducted by Zeb et al. (2008). In our study, the majority of patients admitted for solid tumors received cisplatin chemotherapy weekly for consecutive 2–7 cycles, which was based on tumor type and grading following the protocols. Treatment was initiated in 500-ml sodium chloride 0.9% over 1 hour as per the pre- and post-hydration protocol (mannitol 20% 200 ml infused for 30 minutes and sodium chloride 0.9% + 2 g MgSO4 + 20 mmol KCl 1,000 ml for 2 hours). Urine output was measured (>100 ml/hour) prior to slow administration of cisplatin intravenously. A single dose of furosemide (20 mg) was administered intravenously, if necessary (Pignon et al., 2007). Inj Granisetron 3 mg and Inj Dexamethasone (12 mg) were administered to all patients by intravenous route. In this study, out of 105 patients, 2 patients were treated with Inj Cisplatin (50 mg IV) + Methotrexate (15 mg IV) (monthly cycle for 3 months) for CA Maxilla and 1 patient was treated with Inj Cisplatin (50 mg IV) + Inj Gemcitabine (1.5 gm IV) for CA of gallbladder (every 21-day cycle for 3 cycles). The main adverse effects noted in the study participants were nausea and vomiting nephrotoxicity, myelosuppression (thrombocytopenia), ototoxicity (tinnitus and hearing loss), taste alteration, and other adverse effect. The most frequent adverse effects of cancer chemotherapy medications are nausea and vomiting, particularly when using cisplatin. In most patients receiving cisplatin, nausea and vomiting occur 1–2 hours following chemotherapy if appropriate antiemetic prophylaxis is not administered. The mechanism of action relates to both the central action of these drugs on the chemoreceptor trigger zone (CTZ) and peripheral action in the GI tract. These drugs cause damage to the intestinal mucosa by releasing 5-HT3. The CTZ and vomiting center are activated when this region connects to its receptors on vagal afferent neurons. An intense episode of vomiting is triggered by the release of several neurotransmitters when CTZ is activated. This justified the use of 5HT3 antagonist as prophylaxis against vomiting caused by cisplatin. Thus, 5-HT3 receptor antagonists, such as granisetron, were found to be superior and have been included in the protocol (Ranganath et al., 2015). Granisetron works well against chemotherapy-induced nausea and vomiting when given with dexamethasone prior to highly emetogenic treatment (Bremer 1992). This efficacy is comparable to that of granisetron alone during the acute phase of the condition (Saito et al., 2009). Acute emesis can be adequately controlled when intravenous granisetron and dexamethasone are combined (86% protection) (Aapro et al., 2003). In this study, the severity of vomiting was measured based on nausea and vomiting grading scale NCI CTCAE (Version 4.03) (Gahart et al., 2016). They were categorized as Grade I (39.79 %) and Grade II (31.63%) within 24 hours, and Grade I (55.10%) and Grade II (14.28%) in the delayed type of vomiting. Despite providing each patient with adequate pre-medication in the form of parenteral dexamethasone 12 mg and granisetron 3 mg, the strong emetogenic potential of cisplatin resulted in a high frequency of nausea and vomiting (71.42%). The proportion of vomiting was noted high among our study participants compared with Khandelwal et al. (2015) (41%) (Khandelwal et al., 2015). The nephrotoxicity of cisplatin has been recognized since its introduction over 25 years ago. Cisplatin-induced nephrotoxicity is now well understood. It causes inflammation and injury to renal tubular epithelial cells, leading to apoptosis, and amplifies kidney injury (Miller et al., 2010). This adversity was largely ameliorated by forced pretreatment hydration and chloride diuresis. During the first cycle, nephrotoxicity was noted in 11.22% of the patients, while 17.35% developed during the second cycle and 16.33% and 12.24% developed during the third cycle and fourth cycle, respectively. The decrease in the number of nephrotoxicity during consecutive cycles could be due to post-treatment with mannitol and saline to provide adequate hydration (Brunton and Hilal-Dandan 2018). Cisplatin nephrotoxicity was noted at around 33% in a study conducted by Beyer et al. (1997). Chemotherapy-induced myelosuppression is commonly exhibited as neutropenia, anemia, and thrombocytopenia. Cisplatin has low myelotoxicity because it is relatively less toxic to bone marrow, so transient and mild to moderate thrombocytopenia and leukopenia may occur (Brunton and Hilal-Dandan 2018). In this study, myelosuppression in the form of thrombocytopenia occurred in 39 patients, resulting in a frequency of 39.79%, which is higher than in another study, which reported a frequency of 21% (Zhou et al., 2023). Chattaraj et al. (2023) reported that cisplatin was associated with a 5-fold increased risk of ototoxicity or hearing damage, which can cause ringing in the ears (tinnitus), high-frequency hearing loss, and eventually a reduction in the ability to hear conversation. Tinnitus is known to occur due to electrolyte disturbances, such as hypomagnesemia, hyponatremia, hypocalcemia, and hypokalemia. Of the 98 participants, 18.36% developed tinnitus after the first cycle and the same continued at the end of fourth cycle. A higher proportion of tinnitus (36%) was noted in a study conducted by Chattaraj et al. (2023) The frequency of tinnitus rises with age and is a subjective phenomenon that is challenging to assess objectively. Because it can only measure, quantitate, and describe patient reactions, the results of different studies can vary accordingly (Han et al., 2009). Tinnitus and high-frequency hearing loss are symptoms of cisplatin-induced ototoxicity that are not affected by diuresis. Out of 98 participants, 44.89% developed various types of loss of taste that occur after the patients take chemotherapy at their home. When results were compared to another study, it showed lower results (27%) (Khandelwal et al., 2015). Diarrhea was noted among 12.24% of participants and the incidence was lower compared to other studies (25%) (Khandelwal et al., 2015). Causality analysis of ADR in these patients was based only on the analysis of adverse events. The ADRs were monitored according to published data and textbooks. Rechallenge and dechallenge for causality analysis were not possible and were ethically questionable for these patients. In terms of ADR preventability, myelosuppression, nephrotoxicity, and vomiting were all definitely preventable. Hearing loss, taste loss, and tinnitus were not preventable. In another study, most ADRs were classified as “not preventable”. However, more common reactions, such as nausea and vomiting, belong to the category of “definitely preventable.” Nevertheless, patients experienced vomiting even with the prophylactic use of granisetron and dexamethasone. This might have been reduced to zero with concurrent administration of the newly introduced antiemetic, aprepitant, and its analogs. However, this has not yet been included in the protocol (Pignon et al. 2007) because of the cost factor. Therefore, we did not have a scope for comparison. In our study, all adverse effects were assessed according to Hartwig severity. It was noted that most of the side effects were mild (levels 1 and 2) so that there was no compelling need to alter or stop taking the medication. However, some events of nephrotoxicity, vomiting, and generalized itching were noted as moderate (level 3). In a study conducted by Khandelwal et al. (2015), they noted similar results that most reactions were of “mild level 1” severity, except for vomiting and diarrhea (“moderate level 3”) according to the modified Hartwig and Siegel scale of severity assessment (Khandelwal et al., 2015). A total of 7 patients were excluded from the study because of loss to follow-up and poor compliance, including 3 patients who were taking methotrexate and gemcitabine with cisplatin chemotherapy monthly and every 21-day cycle, respectively. In this study, we could not identify ADRs related to gemcitabine and methotrexate for two reasons. A few percent of patients were receiving concurrent medications, which may increase the risk of drug–drug interactions and change the pharmacokinetics of chemotherapy, increasing the incidence of adverse drug reactions. These patients were lost to follow-up, and it can be difficult to recognize them due to overlapping ADRs (Hanigan et al., 2011). However, in this study, patients who have experienced ADR were mostly taking cisplatin alone and a few in combination with methotrexate and gemcitabine. We could not find any such events in our study, perhaps because the treatment was completely based on the cancer treatment protocol. Very few studies have been conducted in this region, which can emphasize the importance of ADR pattern with cisplatin. In addition, the present study had certain limitations such as attrition, challenges of assessment of differentiation of ADRs between the drugs with combination, and being a single center study, which affected generalizability due to different demographics and limited sample size. ConclusionChemotherapy based on cisplatin carries a significant risk of causing a variety of adverse reactions in patients with cancer. The majority of adverse drug reactions in this study were mild but not preventable; thus, they had no impact on the course of treatment. Notably, certain adverse effects, such as tinnitus and hearing loss, were not preventable, although common adverse effects, such as nausea and vomiting, were preventable. Nephrotoxicity and thrombocytopenia were probably preventable. Conflict of interestNone-declared. FundingNil. Author’s contributionAll authors are involved in each research step. The specific contributions are as follows.
ReferencesAapro, M.S., Thuerlimann, B., Sessa, C., de Pree, C., Bernhard, J. and Maibach, R. 2003. A randomized double-blind trial to compare the clinical efficacy of granisetron with metoclopramide, both combined with dexamethasone in the prophylaxis of chemotherapy-induced delayed emesis. Ann. Oncol. 14, 291–297; 10.1093/annonc/mdg075 Aruna, D.S., Prasad, K.V.V., Shavi, G.R., Ariga, J., Rajesh, G. and Krishna, M. 2011. Retrospective study on risk habits among oral cancer patients in karnataka cancer therapy and research institute, hubli, India. Asian Pacific J. Cancer Prev. 12, 1561–1566. Attia, N. 2017. International Journal of Current Advanced Research. Notes. 1, 444. Barabas, K., Milner, R., Lurie, D. and Adin, C. 2008. Cisplatin: a review of toxicities and therapeutic applications. Vet. Comp. Oncol. 6, 1–18; 10.1111/j.1476-5829.2007.00142.x Bellare, P.S., Ashwin, K., Pu, S.P., Vinaykumar, S. and KB, R. 2016. Retrospective evaluation of adverse drug reactions due to cancer chemotherapy in a tertiary care hospital in South India. J. Young Pharm. 8, 251–254; 10.5530/jyp.2016.3.14 Beyer, J., Rick, O., Weinknecht, S., Kingreen, D., Lenz, K. and Siegert, W. 1997. Nephrotoxicity after high-dose carboplatin, etoposide and ifosfamide in germ-cell tumors: incidence and implications for hematologic recovery and clinical outcome. Bone Marrow Transplant. 20, 813–819; 10.1038/sj.bmt.1700980 Borse, V., Konwar, A.N. and Buragohain, P. 2020. Oral cancer diagnosis and perspectives in India. Sensors Int. 1, 100046; 10.1016/j.sintl.2020.100046 Bremer, K. 1992. A single-blind study of the efficacy and safety of intravenous granisetron compared with alizapride plus dexamethasone in the prophylaxis and control of emesis in patients receiving 5-day cytostatic therapy. Eur. J. Cancer. 28, 1018–1022; 10.1016/0959-8049(92)90446-9 Brunton, L. and Hilal-Dandan, R. 2018. Goodman & Gilman’s The pharmacological basis of Therapeutics. Chennai, India: Mc Graw Hill Education. Chattaraj, A., Syed, M.P., Low, C.A. and Owonikoko, T.K. 2023. Cisplatin-induced ototoxicity: a concise review of the burden, prevention, and interception strategies. JCO Oncol. Pract. 19, 278–283; 10.1200/op.22.00710 Coelho, K.R. 2012. Challenges of the oral cancer burden in India. J. Cancer Epidemiol. 2012, 701932; 10.1155/2012/701932 Dasari, S. and Bernard Tchounwou, P. 2014. Cisplatin in cancer therapy: molecular mechanisms of action. Eur. J. Pharmacol. 740, 364–378. 10; 1016/j.ejphar.2014.07.025 Gahart, B.L., Nazareno, A.R. and Ortega, M.Q. 2016. Appendix C – U.S. department of health and human services, national institutes of health, national cancer institute common terminology criteria for adverse events (CTCAE). 2016 Intraven Medicat. Published Online First: 2016. Ganesan, P., Schmiedge, J., Manchaiah, V., Swapna, S., Dhandayutham, S. and Kothandaraman, P.P. 2018. Ototoxicity: a challenge in diagnosis and treatment. J. Audiol. Otol. 22, 59–68; 10.7874/jao.2017.00360 Gupta, P.C., Murti, P.R. and Bhonsle, R.B. 1996. Epidemiology of cancer by tobacco products and the significance of TSNA. Crit. Rev. Toxicol. 26, 183–198; 10.3109/10408449609017930 Han, B.I., Lee, H.W., Kim, T.Y., Lim, J.S. and Shin, K.S. 2009. Tinnitus: characteristics, causes, mechanisms, and treatments. J. Clin. Neurol. 5, 11. Hanigan, M.H., Dela Cruz, B.L., Shord, S.S., Medina, P.J., Fazili, J. and Thompson, D.M. 2011. Optimizing chemotherapy: concomitant medication lists. Clin. Pharmacol. Ther. 89, 114–119; 10.1038/clpt.2010.253 Hartwig, S.C., Siegel, J. and Schneider, P.J. 1992. Preventability and severity assessment in reporting adverse drug reactions. Am. J. Hosp. Pharm. 49, 2229–2232; 10.1093/ajhp/49.9.2229 Khandelwal, S., Bairy, K.L., Vidyasagar, M.S., Chogtu, B. and Sharan, K. 2015. Adverse drug reaction profile of cancer patients on chemotherapy in a tertiary care hospital. Int. J. Pharma. Bio. Sci. 6, P233–244; doi.org/10.4103/0253-7613.62412 Krishna, A., Singh, R.K., Singh, S., Verma, P., Pal, U.S. and Tiwari, S. 2014. Demographic risk factors, affected anatomical sites and clinicopathological profile for oral squamous cell carcinoma in a north Indian population. Asian Pacific J. Cancer Prev. 15, 6755–6760; 10.7314/APJCP.2014.15.16.6755 Makrilia, N., Syrigou, E., Kaklamanos, I., Manolopoulos, L. and Saif, M.W. 2010. Hypersensitivity reactions associated with platinum antineoplastic agents: a systematic review. Met. Based Drugs 2010, 207084; 10.1155/2010/207084 McSweeney, K.R., Gadanec, L.K., Qaradakhi, T., Ali, B.A., Zulli, A. and Apostolopoulos, V. 2021. Mechanisms of cisplatin-induced acute kidney injury: pathological mechanisms, pharmacological interventions, and genetic mitigations. Cancers (Basel). 13, 1572; 10.3390/cancers13071572 Megari, K. 2013. Quality of life in chronic disease patients. Heal. Psychol. Res. 1, 27; 10.4081/hpr.2013.e27 Miller, R.P., Tadagavadi, R.K., Ramesh, G. and Reeves, W.B. 2010. Mechanisms of cisplatin nephrotoxicity. Toxins (Basel). 2, 2490–2518; 10.3390/toxins2112490 Pignon, J.P., Le Maitre, A. and Bourhis, J. 2007. Meta-analyses of chemotherapy in head and neck cancer (MACH-NC): an update. Int. J. Radiat. Oncol. Biol. Phys. 69, S112–S114. Ranasinghe, R., Mathai, M.L. and Zulli, A. 2022. Cisplatin for cancer therapy and overcoming chemoresistance. Heliyon. 2022, 8; 10.1016/j.heliyon.2022.e10608 Ranganath, P., Einhorn, L. and Albany, C. 2015. Management of chemotherapy induced nausea and vomiting in patients on multiday cisplatin based combination chemotherapy. Biomed. Res. Int. 2015, 943618; 10.1155/2015/943618 Saito, M., Aogi, K., Sekine, I., Yoshizawa, H., Yanagita, Y., Sakai, H., Inoue, K., Kitagawa, C., Ogura, T. and Mitsuhashi, S. 2009. Palonosetron plus dexamethasone versus granisetron plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a double-blind, double-dummy, randomised, comparative phase III trial. Lancet Oncol. 10, 115–124; 10.1016/S1470-2045(08)70313-9 Zhou, S., Song, B., Li, C., Tang, W., Zhang, X., Jin, X., Xu, X., Wang, Q., Zheng, H. and Fu, J. 2023. The predictive model for risk of chemotherapy-induced thrombocytopenia based on antineoplastic drugs for solid tumors in eastern China. Sci Rep. 13, 3185; 10.1038/s41598-023-27824-9 Zeb, A., Rasool, A. and Nasreen, S. 2008. Cancer incidence in the Districts of Dir (North West Frontier Province), Pakistan: a preliminary study. J. Chinese Med. Assoc. 71, 62–65; 10.1016/S1726-4901(08)70076-5 | ||
| How to Cite this Article |
| Pubmed Style Udhnawala HJ, Mirza N, Asarawala N, Ganguly B. Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. Natl J Physiol Pharm Pharmacol. 2025; 15(2): 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 Web Style Udhnawala HJ, Mirza N, Asarawala N, Ganguly B. Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. https://www.njppp.com/?mno=224783 [Access: June 26, 2026]. doi:10.5455/NJPPP.2025.v15.i2.3 AMA (American Medical Association) Style Udhnawala HJ, Mirza N, Asarawala N, Ganguly B. Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. Natl J Physiol Pharm Pharmacol. 2025; 15(2): 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 Vancouver/ICMJE Style Udhnawala HJ, Mirza N, Asarawala N, Ganguly B. Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. Natl J Physiol Pharm Pharmacol. (2025), [cited June 26, 2026]; 15(2): 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 Harvard Style Udhnawala, H. J., Mirza, . N., Asarawala, . N. & Ganguly, . B. (2025) Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. Natl J Physiol Pharm Pharmacol, 15 (2), 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 Turabian Style Udhnawala, Hiren Jitendra, Nazima Mirza, Nirav Asarawala, and Barna Ganguly. 2025. Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. National Journal of Physiology, Pharmacy and Pharmacology, 15 (2), 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 Chicago Style Udhnawala, Hiren Jitendra, Nazima Mirza, Nirav Asarawala, and Barna Ganguly. "Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital." National Journal of Physiology, Pharmacy and Pharmacology 15 (2025), 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 MLA (The Modern Language Association) Style Udhnawala, Hiren Jitendra, Nazima Mirza, Nirav Asarawala, and Barna Ganguly. "Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital." National Journal of Physiology, Pharmacy and Pharmacology 15.2 (2025), 128-136. Print. doi:10.5455/NJPPP.2025.v15.i2.3 APA (American Psychological Association) Style Udhnawala, H. J., Mirza, . N., Asarawala, . N. & Ganguly, . B. (2025) Range of adverse drug reactions in patients on cisplatin-based cancer chemotherapy in a tertiary care hospital. National Journal of Physiology, Pharmacy and Pharmacology, 15 (2), 128-136. doi:10.5455/NJPPP.2025.v15.i2.3 |

